
Surveillance of chronic kidney disease (CKD) risk group patients
The civilisation diseases diabetes, hypertension and obesity are the main drivers of the development of chronic kidney disease. The increasing prevalence of these diseases during the last thirty years positively correlates with an increase in the prevalence of chronic kidney disease, reaching 9.1 % in 2017.
Chronic kidney disease diminishes the quality of life of patients, especially at a later stage when CKD progresses into end-stage renal failure and renal replacement therapies (RRT) become necessary. High healthcare expenditures and socio-economic disadvantages are additional consequences.
Since the development of CKD can be reverted or its progression slowed down if detected at an early stage, a regular screening of risk patients for the onset of CKD can help to ease the burden and fight CKD.
The challenge
Caring for patients suffering from civilisation diseases not only means maintaining their condition and monitoring their treatment. Continuous surveillance such as looking out for and managing corresponding secondary diseases poses an additional challenge. Limited healthcare budgets and cost-intensive diagnostics have so far prevented a broad and frequent screening of risk groups.
DETECTING THE ONSET OF CKD
Early detection of the onset of CKD in risk group patients
Following KDIGO guidelines, estimated glomerular filtration rate (eGFR) and albuminuria are the key diagnostic tools for detecting chronic kidney disease. Since moderately increased albuminuria is an early indicator of chronic kidney disease at a reversible stage, regular albuminuria screening of risk groups could be a proper procedure in managing patients suffering from civilisation diseases.
While cost-intensive diagnostic methods such as sensitive and quantitative immunonephelometry are not suitable for this, a routine urine test strip test has now reached a sensitivity and accuracy comparable to that of immune-based assays.
9.1% prevalence of chronic kidney disease, continuously increasing since 1990.
COST-EFFICIENT SCREENING
Enabling a regular screening of CKD risk groups
Albuminuria and the albumin:creatinine ratio can now be detected even at low concentrations in a cost-efficient way, allowing a frequent and broad screening of CKD-related risk groups. This allows to either avoid unnecessary diagnostics or to initiate specific follow-up, and treatment adjustment can be initiated early on to halt or slow down the progression of CKD.
With the progression of CKD we see today, the annual socio-economic cost will amount to € 84 billion. Individual annual CKD treatment cost may be as high as € 90,000 (stage V of the disease).
36 million disability-adjusted life-years (DALYs) are accumulated among CKD patients.
SCREENING AT THE POINT OF CARE
Screening for chronic kidney disease at the point of care
General practitioners look after the majority of patients suffering from civilisation diseases. This includes the diagnosis as well as treatment monitoring.
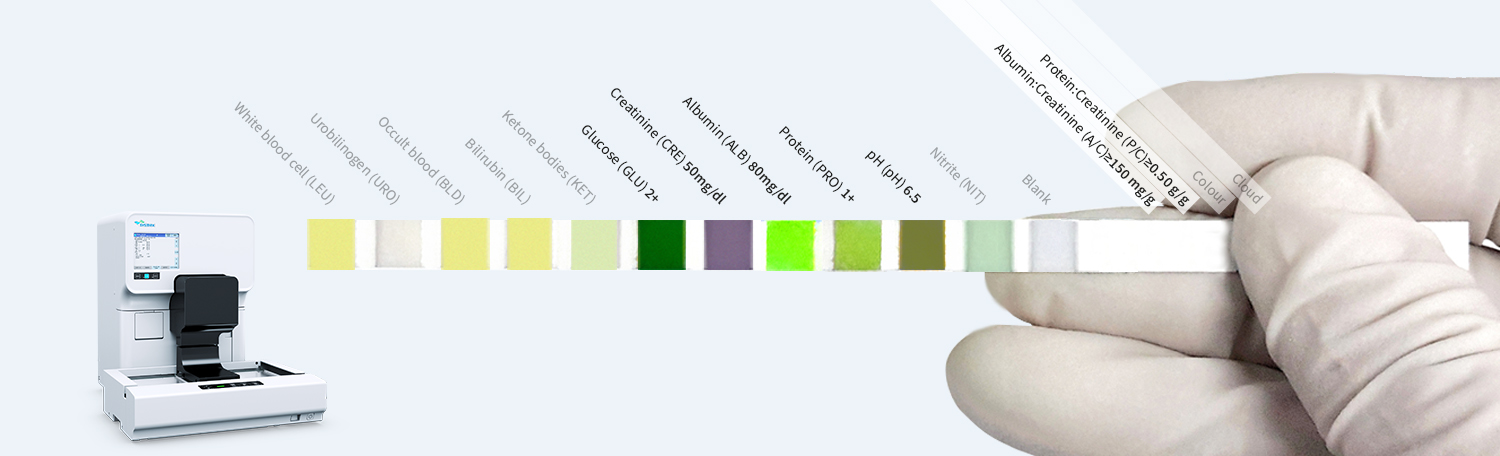
The accurate and automated detection of albuminuria and elevated albumin:creatinine ratios from a test strip is not only possible in a routine laboratory setting, but also at the point of care, using test strips in combination with the semi-automated test strip reader UC-1000. This allows general practitioners to frequently screen their patients at risk of CKD without compromising on sensitivity – there’s no direct need for special immune-based tests.
5.4 million people will require RRT (renal replacement therapy) by 2030.

Clinical case examples
Clinical case examples
Progression of CKD: early diagnosis is key
A 68-year-old patient suffering from a long history of obesity and diabetes mellitus presented himself for a routine check-up. Due to persistent hyperglycaemia, test strip analysis of a urine sample was performed, pointing out moderately increased albuminuria and elevated urinary protein levels.
When correlated to urinary creatinine levels, this increase showed itself also in the albumin:creatinine and protein:creatinine ratios. While there were no signs of haematuria, urine particle analysis revealed the presence of renal tubular epithelial cells.
Publications
Delanghe JR, Himpe J, De Cock N, Delanghe S, De Herde K, Stove V and Speeckaert MM (2017) Sensitive albuminuria analysis using dye-binding based test strip. Clin Chim Acta 471:107-112
GBD Chronic Kidney Disease Collaboration (2020) Global, regional, and national burden of chronic kidney disease 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 395(10225):709-733
Forouzanfar MH et al. (2017) Global Burden of Hypertension and Systolic Blood Pressure of at Least 110 to 115mmHg, 1990-2015. JAMA 317(2):165-18
Khan MAB, Hashim MJ, King JK, Govender RD, Mustafa H and Al Kaabi J (2020) Epidemiology of Type 2 Diabetes – Global Burden of Disease and Forecasted Trends. Journal of Epidemiology and Global Health 10(1):107–111
Salínas M, López-Garrigós M, Flores E, Lugo J, Leiva-Salínas C and PRIMary Care-LABoratory (PRIMLAB) working group (2018) Urinary albumin strip assay as a screening test to replace quantitative technology in certain conditions. Clin Chem Lab Med 57(2):204-209


